Quality rounds have been rolled out across 16 units at our academic medical centers. They recently launched on three Salem Hospital units and are launching today on three Newton-Wellesley Hospital units as well. Rounds will eventually be adopted systemwide.
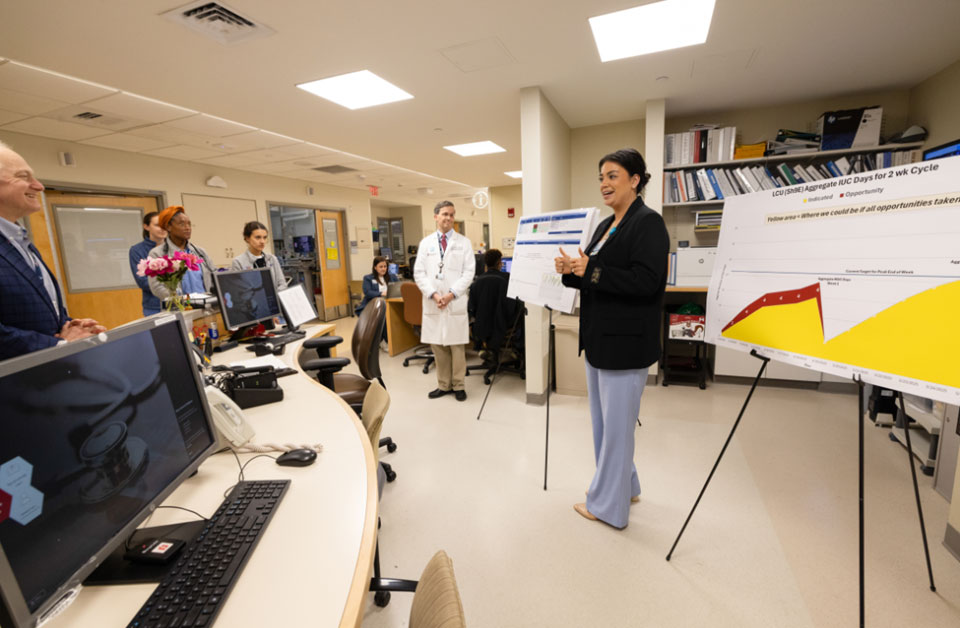
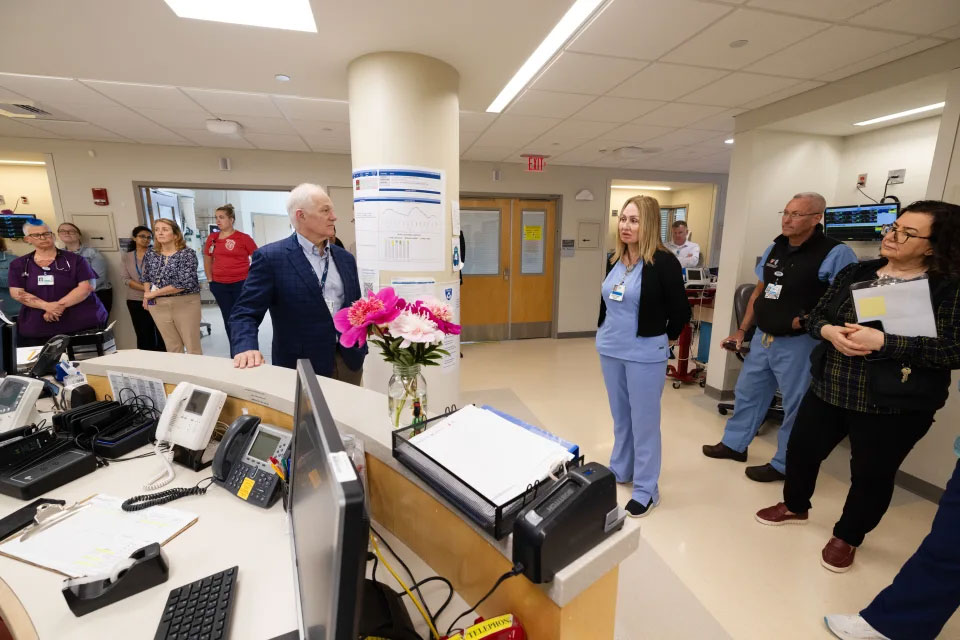
Held every other week, rounds bring together frontline clinicians and staff with hospital and system leaders to review a unit’s own data, which is displayed on a “scorecard” that tracks risks across a series of metrics that are key to improving patient outcomes, experience, equity and the overall care we provide.
During these huddles, staff can identify challenges related to patient progression, share ideas for improvement and then help operationalize proposed solutions.
For general care units, Patient Care Progression uses a unit’s discharge rate to measure length of stay. A validated metric that has been implemented successfully at MGB and other health systems, the rate correlates closely with length of stay.
“The data provide transparency that is helping our care teams identify risk and work together on solutions to improve outcomes for our patients,” Vazza said. “Ideally, quality rounds will become an incubator for the best new ideas and practices, like the improvement initiative on Blake 8, that could eventually be spread systemwide.”
A great outcome
On Blake 8, a Cardiac Surgical ICU at Massachusetts General Hospital (MGH), rounds sparked a collaboration between the unit’s physicians, advanced practice providers and nurses who together focused on eliminating delays in transferring patients to step-down units.
The teams established nightly, cross-team communication to help identify and prepare patients who were ready to have chest tubes and wires removed. Eligible patients are now ready for transfer by 10 a.m. each day. As a result, Blake 8’s length-of-stay performance improved from 1.6 days to .9 days (target is 1 day) within three months, highlighting the success of the unit’s multidisciplinary intervention.
“Rounds are bringing the unit together as a team,” said Megan Tibbetts, CNP, who is leading the improvement initiative in collaboration with unit Medical Director Aranya Bagchi, MBBS, and Nursing Director Vivian Donahue, RN. “Colleagues in every role are invested in improving outcomes for our patients, and it’s great to see we’re making an impact.”
Equipping teams with the tools they need
Every unit participating in quality rounds receives a tool kit of resources for each role group (provider, nurse and case manager) that can be used to support patient progression.
Nurses, for example, receive tip sheets on the assessment and management of delirium and mobility. These tools, designed by our system’s nursing leaders, guide staff on how to use nationally validated methodologies to support delirium care and increase patient mobility.
Mobility guidance was developed by nursing and physical therapy leaders, incorporating best practices already in place at our community hospitals. It includes a validated mobility assessment tool that assigns patients a mobility score on admission. The score improves early identification of post-acute care needs and reduces unnecessary physical therapy consults, which can further prolong care.
“We are using data to predict what patients’ needs will be and initiate earlier Case Management involvement to assist with care transitions,” said Debra Burke, RN, DNP, MBA, NEA-BC, senior vice president of Patient Care Services and chief nursing officer at MGH.
“We are creating a culture where everyone who is taking care of patients is thinking about mobility,” said Reg B. Wilcox III, PT, DPT, MS, MBA, OCS, executive director of Rehabilitation at Brigham and Women’s Hospital and Brigham and Women’s Faulkner Hospital. “Mobility scoring by our nurses is an important step in that process.”
“Quality rounds provide a powerful opportunity for continual learning, collaboration and improvement,” Safavi said. “That’s what is so exciting about becoming a High Reliability Organization.”